I would be very hesitant to speculate about causality. At the moment, anything beyond data collection and ruling out confounders is most likely aligned with a political agenda of some sort.
Here is a paper (gated, but Medscape allows free registration)
Loss of smell. Fatigue. Mental health challenges. Difficulty breathing and other lower respiratory diseases. Fluid and electrolyte disorders. Cardiac dysrhythmia and other nonspecific chest pains. Trouble with urination. Diabetes?
Statistically, these are the conditions that defined post-acute SARS-CoV-2 (PASC) infection, or long COVID, for 28,118 people who tested positive for SARS-CoV-2 by PCR before the Omicron wave. The data, presented at the Conference on Retroviruses and Opportunistic Infections 2022, can be used to guide diagnoses of long COVID, and may be the guide soon at Kaiser Permanente offices, said Michael Horberg, MD, executive director of research, community benefit, and Medicaid strategy at the Mid-Atlantic Permanente Research Institute, in an interview with Medscape Medical News.
“There are some real conditions you could ask about” if you were evaluating a patient who believes they have PASC, Horberg said. “And there are real conditions that are symptoms patients have but they don’t fit the PASC diagnosis.”
Given how much propaganda surrounded the COVID-19 response in most Western countries, it’s not surprising to see conditions like the so-called “long COVID” emerge. Some people speculate that given its broad list of vague symptoms and imprecise differential diagnostic, long COVID is similar to CFS (chronic fatigue syndrome), which itself was surrounded by controversy as to whether it has real underlying physiological causes (link)
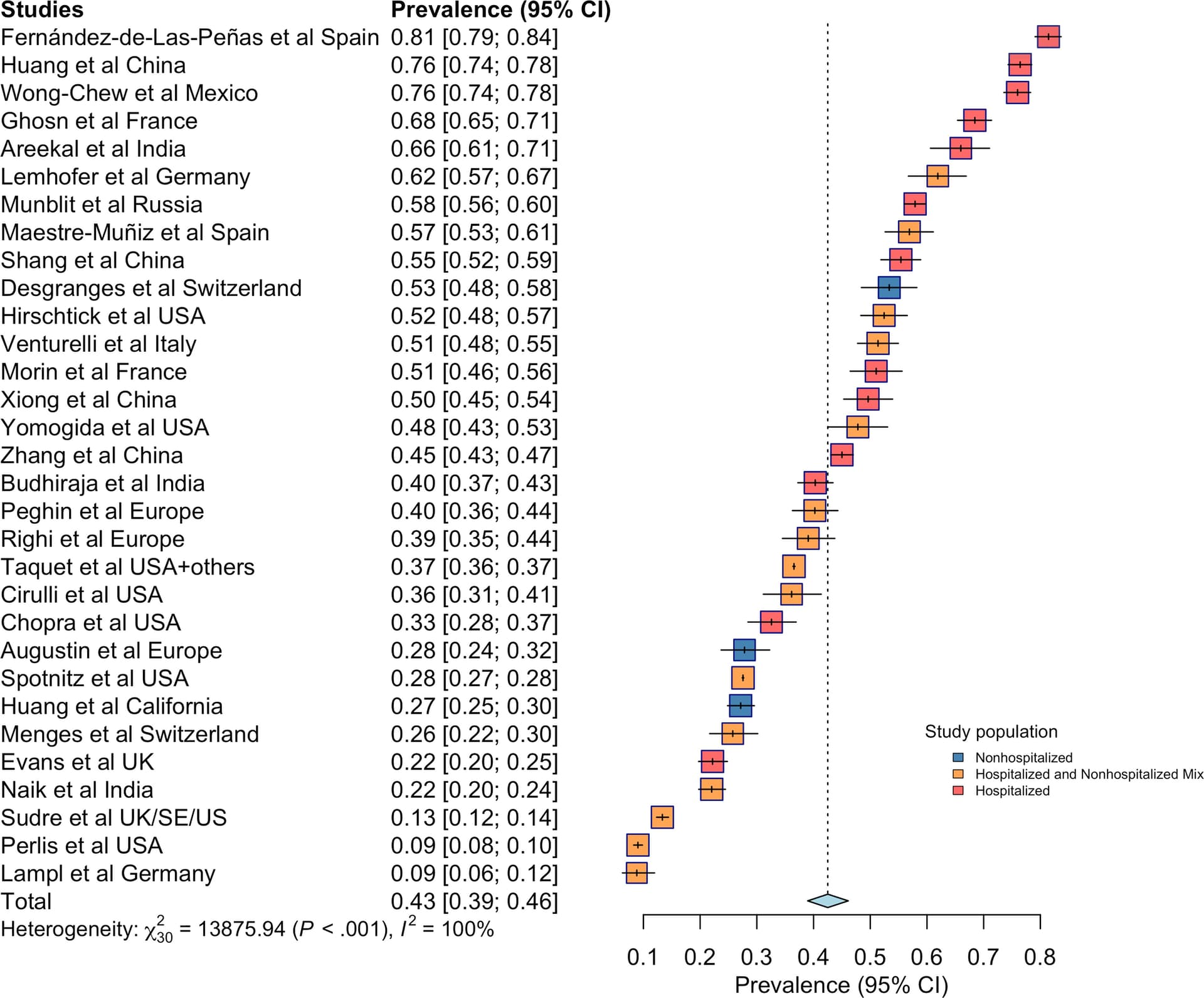
An April 2022 meta-analysis of long COVID occurrence found that estimates ranged widely from 0.09% to 0.81% (The Journal of Infectious Diseases)
Forest plot for worldwide post-coronavirus disease 2019 condition prevalence. Prevalence estimates and 95% confidence intervals (CIs) are provided for each study with a relevant measure and for the meta-analysis of all such studies. For individual studies, the horizontal line represents the estimate, whiskers represent the CI, the size of the box represents the weight assigned to the study, and the color shading reflects the hospitalization status of the study population, as noted in the legend. For the pooled estimate, the width of the diamond represents the CI. Meta-analyzed prevalence and 95% CIs are calculated using random-effects models with inverse variance weighting as described under Methods. Measures of heterogeneity of prevalence estimates are provided.
My take is that something a) imprecisely defined, with b) widely varying prevalence, and c) that stands to directly benefit the so-called health care industry (pharma + medical profession) ought to be met with skepticism.